AI-Powered Medical Diagnostic System for Spine and Chest Pathology Detection
Built to reduce diagnostic delays in emergency radiology by detecting cervical fractures and chest pathologies with 99% accuracy.
Spine Accuracy
99.1%
Inference Speed
41ms
Time-to-Diagnosis Cut
70%
When Radiology Workflows Could No Longer Keep Up With Emergency Caseloads
In high-volume trauma units, the speed of a diagnosis can determine whether a patient walks out or not. Cervical fractures at C1 through C7 require immediate detection to prevent permanent neurological damage. Pneumonia and related chest opacities need to be caught early in patients who cannot wait for a radiologist to clear a backlog. The problem is not a shortage of clinical expertise. It is a structural one. Modern imaging volumes have outpaced the capacity of manual review, and the consequences of falling behind are clinical, not operational.
Akoode's AI engineering team set out to build a dual-stream Clinical Decision Support System that could process spinal CT scans and chest X-rays in real time, flag critical findings at the top of a radiologist's worklist, and explain its reasoning visually so clinicians could trust and act on the output. The system needed to run at near-instant inference speeds, hit accuracy benchmarks comparable to specialist review, and present findings in a way that reduced cognitive load rather than adding to it.
The result is the Sahayak Diagnostic Orchestrator: a Streamlit-based clinical interface powered by a hybrid EfficientNetV2-B3 and BiGRU deep learning architecture, trained on approximately 500,000 images from NIH and RSNA datasets, capable of processing a full study in 41 milliseconds and delivering vertebra-level fracture risk and chest pathology findings with Grad-CAM attention maps for clinical transparency.
99.1%
Spine Detection Accuracy
Aggregated accuracy across cervical vertebrae C1 through C7 fracture detection on the RSNA validation dataset.
98.4%
Chest Pathology Accuracy
Binary classification accuracy for pneumonia and related chest opacities on the NIH Chest X-ray 14 dataset.
41ms
Inference Speed Per Study
Each radiograph or spinal scan is fully processed in approximately 41 milliseconds on NVIDIA T4 GPU hardware.
70%+
Time-to-Diagnosis Reduction
Diagnostic turnaround time in critical trauma scenarios cut by more than 70% compared to manual review workflows.
Project Info
Client
Confidential, India
Industry
Healthcare
Use Case
Real-Time Clinical Decision Support for Radiology
Solution
Artificial Intelligence and Deep Learning
Engagement
Fixed Cost
What Challenges Do Radiologists Face in High-Volume Emergency Diagnostic Environments?
Radiology departments in emergency and trauma settings are caught between two pressures that pull in opposite directions. Imaging volumes keep rising. The tolerance for missed diagnoses stays at zero. A hairline cervical fracture overlooked during a busy overnight shift, or a pneumonia finding buried halfway down a full worklist, carries consequences that extend well beyond clinical error. Existing AI tools have added a third problem on top of both: they produce outputs without explanation, and clinicians who cannot see why a model flagged something are right to be cautious about acting on it.
Diagnostic Bottlenecks in Trauma Units
Emergency radiologists reviewing high volumes of spinal and chest scans have no automated system to prioritise critical findings, leaving life-threatening conditions in a queue rather than at the top of the worklist.
Hairline Fractures Missed Under High Workload
Subtle cervical fractures are difficult to detect even under optimal conditions. During high-volume shifts, fatigue increases the miss rate for exactly the findings that carry the most immediate clinical risk.
No Transparency in Existing AI Diagnostic Tools
Most AI radiology tools produce a classification without showing where in the image the model focused. Clinicians cannot verify the finding, cannot document it confidently, and are less likely to act on outputs they cannot explain to a patient or colleague.
Volumetric Spinal Data Processed as Flat 2D Slices
Standard models treat each CT slice as an independent image. Cervical fractures often span multiple vertebral levels and require the model to understand the spine as a continuous anatomical structure, which 2D slice-by-slice processing cannot do reliably.
A radiologist reviewing 80 studies in a shift is not less skilled at study 80 than at study one. But the system they work in does not account for that reality. The AI layer needs to catch what human fatigue misses, not just confirm what is already obvious.
What We Set Out to Build
The brief was specific: a dual-stream diagnostic system that could detect cervical spine fractures at individual vertebra level and classify chest pathologies from X-rays, process each study in under two seconds, and present findings with visual explainability that clinicians could act on without second-guessing the model. Accuracy targets were set at specialist-comparable benchmarks. The clinical interface needed to triage automatically, not just classify.
Build Dual-Stream Diagnostic Architecture
Develop two separate but integrated AI streams: one for volumetric cervical spine fracture detection across C1 through C7, and one for chest X-ray pathology classification, unified within a single clinical decision support interface.
Achieve Sub-Two-Second Inference at High Accuracy
Engineer the full inference pipeline to process a complete study in under two seconds at 99% accuracy for spine and 98% for chest, using GPU-optimised mixed precision to maintain speed without sacrificing detection performance.
Implement Explainable AI With Grad-CAM Visualisation
Integrate Grad-CAM attention mapping so every AI finding is accompanied by a heatmap showing exactly which region of the radiograph drove the classification, giving radiologists visual confirmation they can document and act on.
Deliver Automated Triage and Worklist Prioritisation
Build an automated triage layer that flags critical findings immediately with high-visibility alerts, pushing life-threatening cases to the top of the radiologist's worklist rather than presenting all studies in arrival order.
Train on Large-Scale Validated Medical Datasets
Train and validate both models on established, peer-recognised datasets including NIH Chest X-ray 14 and RSNA Cervical Spine Fracture Detection, using a two-phase fine-tuning strategy to prevent weight shattering in the pre-trained backbone.
Turning Raw Radiological Data into Intelligent Clinical Decisions
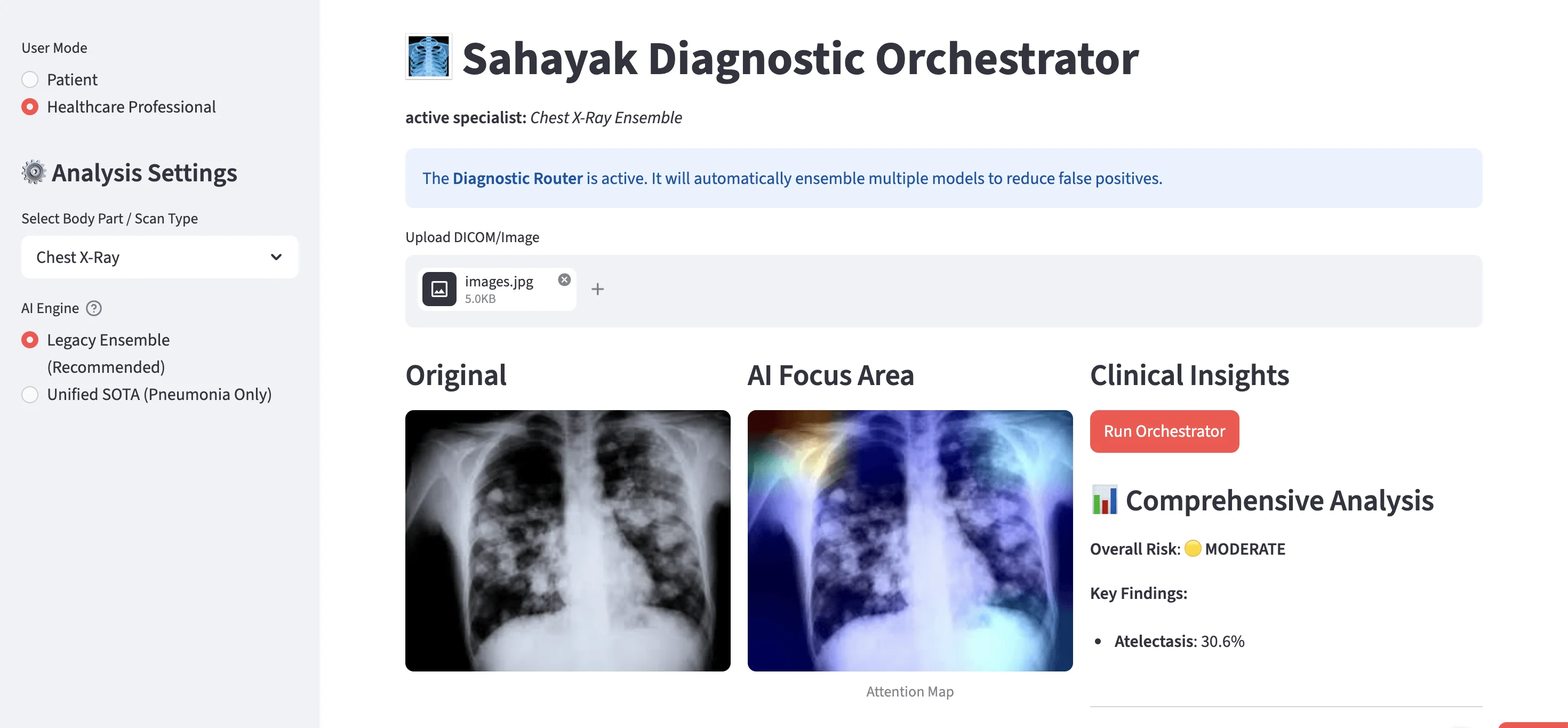
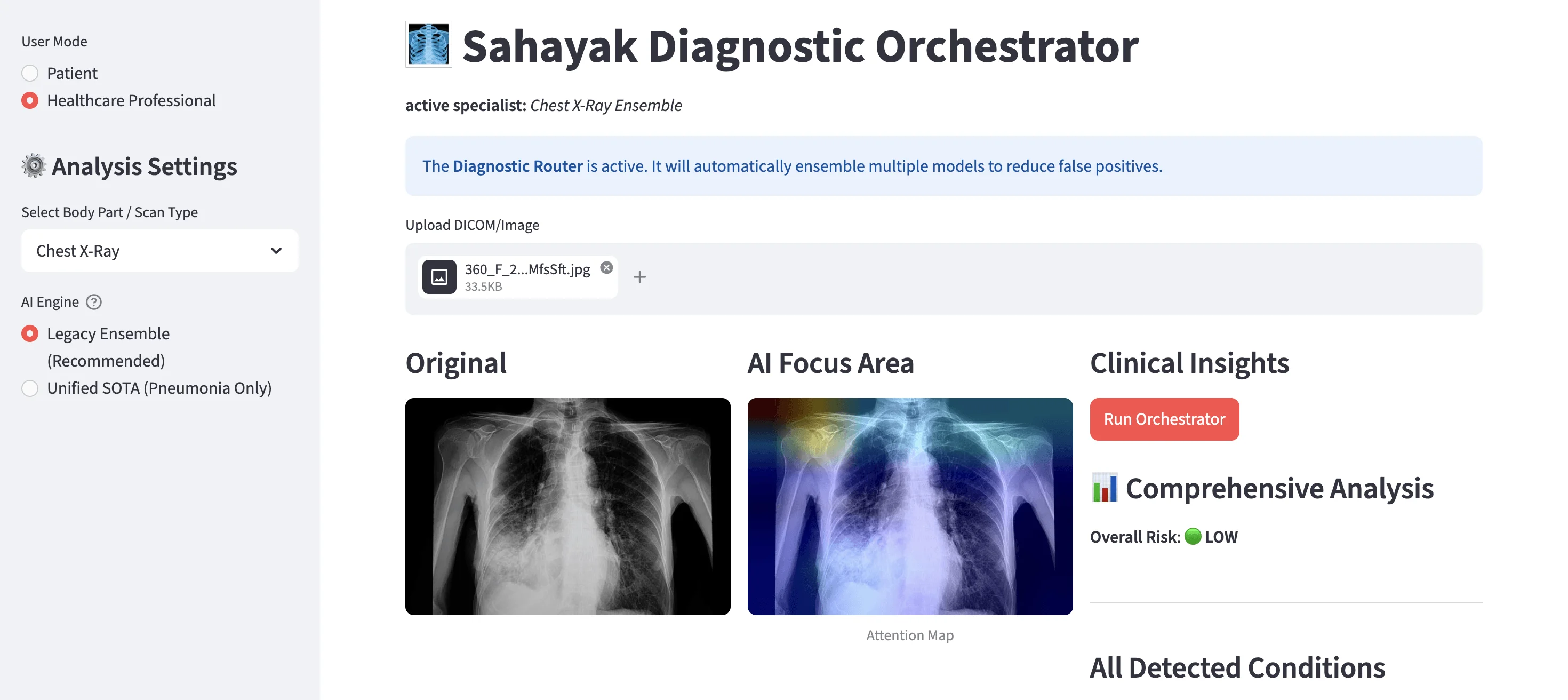
Akoode built the Sahayak Diagnostic Orchestrator as a dual-stream deep learning system combining EfficientNetV2-B3 feature extraction with BiGRU temporal analysis for spine, and ensemble classification for chest. A Grad-CAM attention layer produces visual heatmaps alongside every finding. The Streamlit clinical interface handles automated triage, vertebra-level fracture breakdown, and two-mode operation for patients and healthcare professionals.
Image Ingestion
Radiographs and DICOM files are uploaded directly through the Sahayak interface. CLAHE contrast enhancement and three-channel stacking are applied during preprocessing to improve model sensitivity on low-contrast or compressed imaging inputs.
Dual-Stream AI Analysis
The spine stream processes volumetric data through the hybrid EfficientNetV2-B3 and BiGRU architecture, reading cervical structure as a continuous anatomical sequence rather than independent slices. The chest stream runs ensemble classification across the NIH-trained models, combining multiple outputs to reduce false positives before a finding is surfaced.
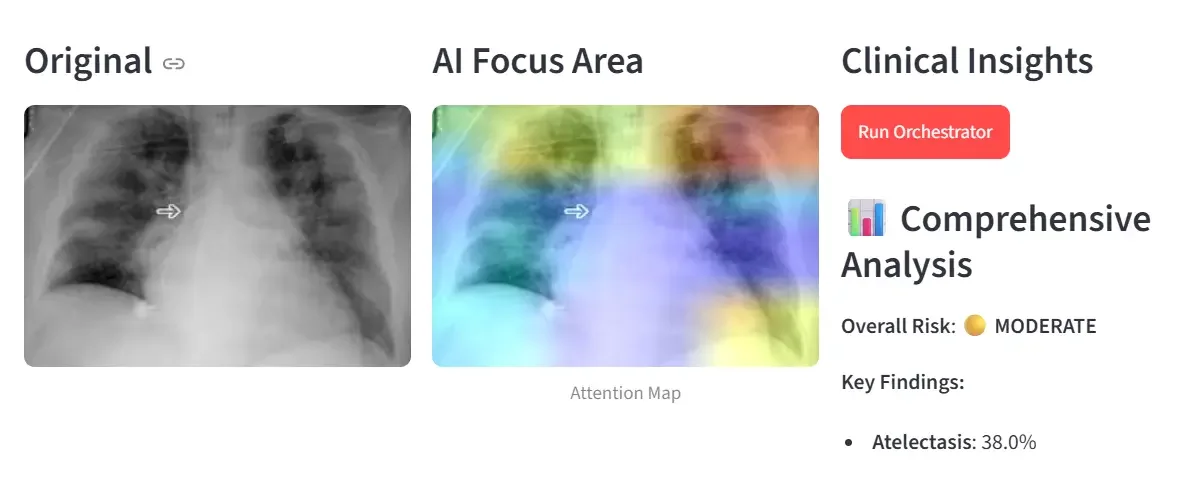
Grad-CAM Attention Mapping
Once classification is complete, Grad-CAM generates a heatmap overlaid directly on the original radiograph, highlighting the specific anatomical region the model focused on. Radiologists see the finding and its location in the same view.
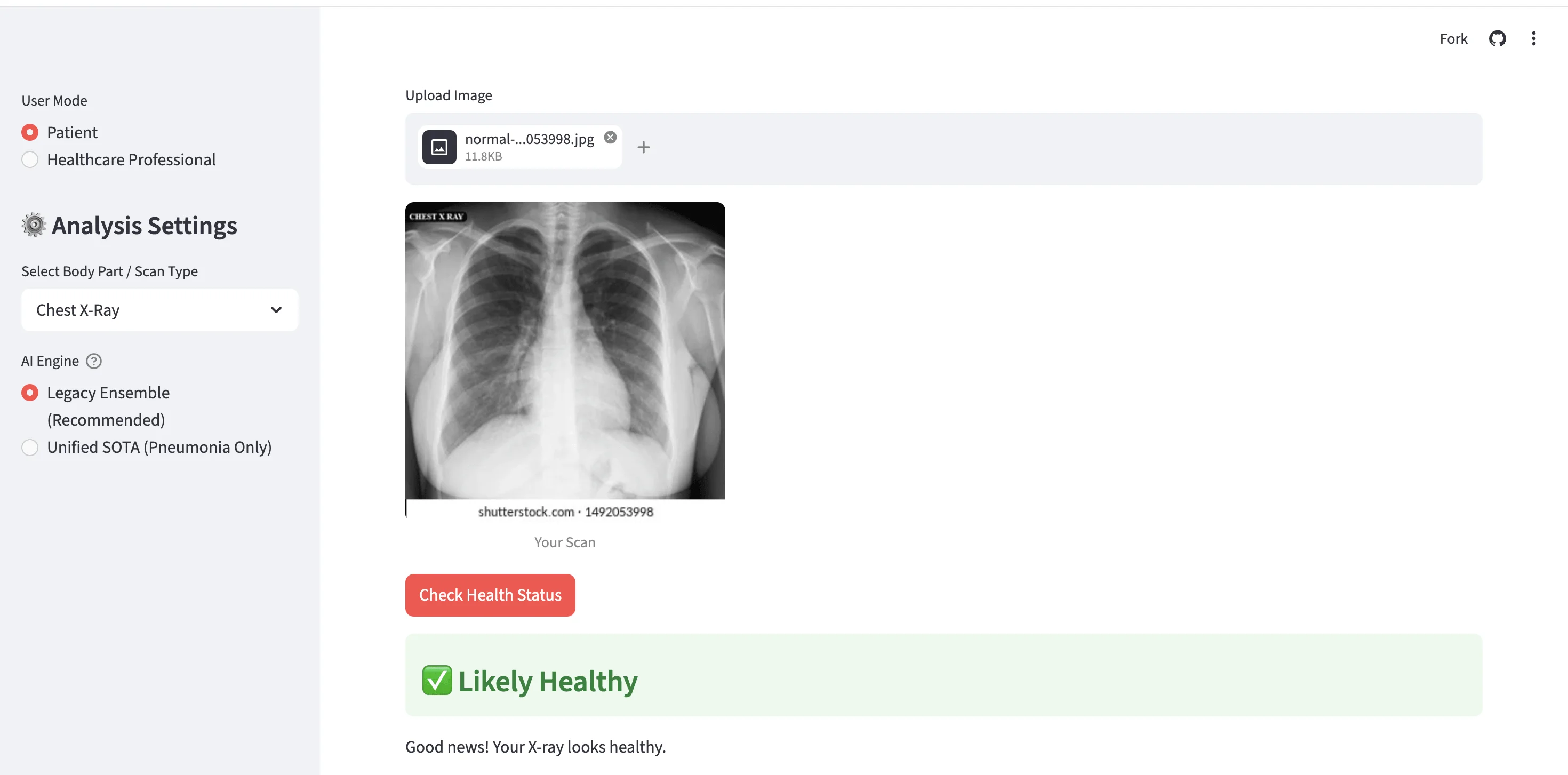
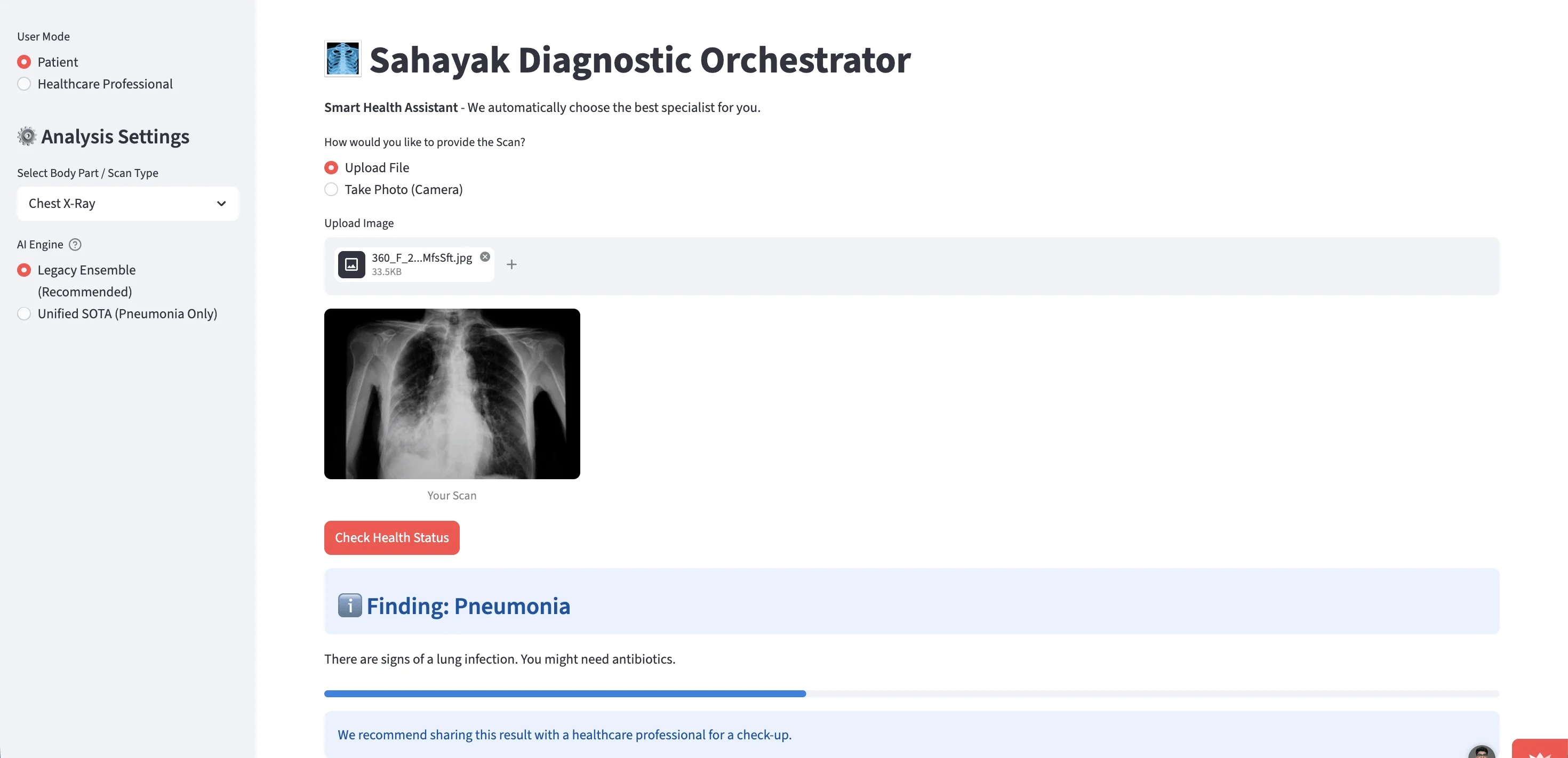
Automated Triage and Alerts
The system assigns each study a risk level and surfaces critical findings immediately. Pneumonia flagged as Critical appears at the top with a high-visibility alert. Likely healthy scans are cleared with a green confirmation. Radiologists see what needs attention first without scrolling through a flat queue.
Clinical Output and Granular Breakdown
For spine studies, fracture risk is reported individually for each vertebra from C1 through C7. For chest, key findings and confidence scores are listed under the risk classification. Both outputs are available in patient mode and healthcare professional mode with appropriate detail levels for each audience.
What Makes This System Powerful
Highlight 01
Hybrid EfficientNetV2-BiGRU Architecture for Volumetric Spine Analysis
Standard object detection models read spinal CT slices one at a time. That misses fractures that span vertebral boundaries or present subtly across a sequence. The Sahayak spine model uses EfficientNetV2-B3 for spatial feature extraction and Bidirectional GRU units for temporal analysis across the slice sequence, treating the cervical spine as a continuous anatomical structure. The result is 99.1% aggregated accuracy across C1 through C7.
- Reads spine as anatomical sequence rather than flat 2D slices
- BiGRU captures cross-vertebra fracture patterns standard models miss
- Vertebra-level risk output for C1 through C7 individually
Highlight 02
Grad-CAM Explainable AI Heatmaps for Clinical Transparency
Every finding the system produces comes with a Grad-CAM attention map overlaid on the original image. The radiologist sees exactly which area drove the classification: the right lower lobe for a pneumonia flag, a specific vertebral level for a fracture risk alert. That transparency is what makes the output usable in a clinical setting rather than just statistically impressive on a benchmark.
- Attention heatmap generated for every finding automatically
- Original and AI focus area shown side by side in the interface
- Clinicians can document and explain findings with visual evidence
Highlight 03
Automated Triage System With Worklist Prioritisation
Studies are not presented in arrival order. The system assigns a risk level to each scan and surfaces critical findings at the top. A critical pneumonia case triggers a high-visibility alert immediately. A likely healthy chest X-ray is cleared with a green confirmation. The radiologist's attention goes to the cases that need it most, not the cases that arrived first.
- Risk-tiered worklist ordering with critical cases surfaced immediately
- High-visibility alerts for life-threatening findings
- Likely healthy scans confirmed and cleared without manual review
Highlight 04
Dual-Mode Clinical Interface for Patients and Healthcare Professionals
The Sahayak Orchestrator runs in two modes. Patient mode delivers plain-language findings: "There are signs of a lung infection. You might need antibiotics." Healthcare professional mode delivers the full clinical output: ensemble model selection, DICOM upload, comprehensive analysis, key findings with confidence percentages, and the attention map. One interface, two appropriate levels of detail.
- Patient mode delivers plain-language findings and next steps
- Professional mode delivers full diagnostic breakdown and ensemble controls
- Streamlit interface accessible without specialist hardware or software installation
Key Challenges in Building an AI Clinical Decision Support System for Emergency Radiology
Medical AI carries a different standard than most software categories. A false negative in a cervical fracture detection system is not a UX problem. Getting from a statistically impressive model to one that a radiologist can actually trust and act on required solving problems in volumetric data processing, inference speed, and clinical transparency that no off-the-shelf configuration addressed cleanly.

Detecting Fractures Across Vertebral Sequences
Cervical fractures often span multiple levels. A model reading each CT slice independently misses the cross-vertebra patterns that carry the most diagnostic weight.
Our Approach
BiGRU units were added after the EfficientNetV2 feature extractor to process slice sequences as continuous anatomical data, giving the model temporal context across the full cervical structure.
Hitting Clinical Accuracy on Imbalanced Datasets
Medical imaging datasets are heavily skewed toward healthy scans. Training on imbalanced data produces models that are good at confirming health and poor at catching pathology.
Our Approach
A two-phase fine-tuning strategy was used to prevent weight shattering in the pre-trained backbone, with CLAHE preprocessing improving model sensitivity on low-contrast inputs before training.
Achieving Sub-41ms Inference Without Accuracy Loss
Reducing inference time typically means simplifying the model. Simplifying the model typically means losing accuracy. Neither option was acceptable.
Our Approach
Mixed precision training using float16 on NVIDIA T4 GPUs maintained model complexity while cutting computational load, delivering 41ms per study without reducing detection performance.
Making AI Outputs Clinically Trustworthy
A classification without explanation is not clinically useful. Radiologists need to see where the model looked, not just what it concluded.
Our Approach
Grad-CAM attention maps were integrated to overlay focus areas directly on the original radiograph, giving clinicians visual confirmation they can document, explain, and act on with confidence.
What Changed After Implementation
Before this system, a radiologist in a busy trauma unit reviewed spinal CT stacks and chest X-rays in arrival order, with no automated layer to surface critical findings first. A hairline cervical fracture on study 60 of an overnight shift received the same priority as a routine chest check. After deployment, every study is processed in 41 milliseconds. Critical cases surface immediately. Hairline fractures that would likely be missed under fatigue are flagged at the vertebra level with a Grad-CAM heatmap showing exactly where to look. Time-to-diagnosis in critical trauma scenarios is cut by over 70%.
No Automated Prioritisation of Critical Findings
Studies reviewed in arrival order with no system to flag life-threatening cervical fractures or critical pneumonia cases to the top of the queue.
Hairline Fractures Vulnerable to Fatigue-Driven Misses
Subtle cervical fractures requiring detection across vertebral sequences had no safety net during high-volume overnight shifts.
AI Tools Producing Unexplained Classifications
Existing diagnostic AI outputs lacked visual confirmation, making findings difficult to trust, document, or act on in a clinical setting.
Volumetric Spine Data Processed as Flat Slices
No model was reading cervical CT stacks as continuous anatomical sequences, missing cross-vertebra fracture patterns that matter most clinically.
Automated Triage With Risk-Tiered Worklist
Critical findings surface immediately with high-visibility alerts. Radiologists see what needs attention first rather than working through a flat queue.
Hybrid BiGRU Architecture for Sequence-Aware Detection
EfficientNetV2-B3 and BiGRU process cervical spine as a continuous anatomical sequence, catching cross-vertebra fractures that slice-by-slice models miss.
Grad-CAM Heatmaps on Every Finding
Attention maps overlay the exact region driving each classification onto the original radiograph, giving clinicians visual evidence they can document and explain.
Two-Phase Fine-Tuning on 500,000 Medical Images
Models trained on NIH and RSNA datasets with CLAHE preprocessing and a two-phase fine-tuning strategy to prevent backbone degradation and improve sensitivity on subtle pathologies.
Critical Cases Reach Radiologists Immediately
Risk-tiered triage surfaces cervical fractures and critical pneumonia findings at the top of the worklist without manual sorting.
99.1% Spine and 98.4% Chest Accuracy Live
Both detection streams running at specialist-comparable accuracy benchmarks on validated clinical datasets.
Every Output Comes With Visual Confirmation
Radiologists receive a finding and a heatmap showing exactly where the model focused, making AI output documentable and clinically defensible.
Time-to-Diagnosis Cut by Over 70%
Full study processed in 41 milliseconds. Diagnostic turnaround in critical trauma scenarios reduced by more than 70% against manual review.
99.1%Spine Detection Accuracy
Aggregated accuracy across C1 through C7 cervical fracture detection on the RSNA validation dataset.
41msInference Speed Per Study
Each radiograph processed in approximately 41 milliseconds on NVIDIA T4 GPU hardware.
70%+Time-to-Diagnosis Reduction
Diagnostic turnaround in critical trauma scenarios cut by more than 70% against manual review workflows.
Use Cases of AI Deep Learning in Medical Imaging and Clinical Decision Support
The dual-stream architecture, explainable AI layer, and automated triage system built for the Sahayak platform applies across any clinical environment where imaging volume, diagnostic speed, and accuracy under pressure are all requirements simultaneously. The same approach works in orthopaedics, pulmonology, oncology screening, and emergency medicine.
Emergency Trauma Unit Spinal Triage
Hospitals handling high volumes of trauma admissions where cervical fracture detection speed directly affects neurological outcomes and treatment decisions.
Chest X-Ray Screening at Scale
Healthcare systems running large-scale respiratory screening programmes where pneumonia, atelectasis, and related opacities need to be flagged automatically across high daily volumes.
Radiology Worklist Prioritisation Systems
Radiology departments managing mixed-acuity imaging queues that need AI-driven triage to ensure critical findings reach a radiologist before routine studies.
Explainable AI for Clinical Documentation
Any healthcare AI application where regulatory or clinical governance requirements demand that AI outputs be visually explainable and documentable by the reviewing clinician.
Remote and Underserved Radiology Support
Hospitals in regions with limited specialist radiology access where an AI clinical decision support layer can provide a level of diagnostic safety net between image capture and specialist review.
Oncology and Pathology Screening Platforms
Cancer screening programmes using deep learning models trained on large validated datasets to detect early-stage findings that carry high miss rates under manual review at scale.
Why Businesses Choose Akoode Technologies for Artificial Intelligence Development
Akoode builds AI systems for healthcare, industrial, and enterprise organisations where accuracy benchmarks, clinical trust, and production-ready deployment are all non-negotiable. The team covers the full scope from model architecture and dataset training through inference optimisation, explainability integration, and clinical interface development. Projects span medical imaging, computer vision, and deep learning applications across India and international markets.
Deep Learning Architecture Designed for Clinical Requirements
The Sahayak system was not built by adapting a general-purpose classification model to a medical problem. The BiGRU temporal layer, the two-phase fine-tuning strategy, and the CLAHE preprocessing pipeline were all chosen specifically because the clinical problem required them. That distinction matters when the accuracy benchmark has patient outcomes attached to it.
Explainability Built Into the Architecture, Not Added After
Grad-CAM integration was part of the system design from the start. It was not retrofitted after a clinician asked why the model flagged something. AI outputs in clinical settings need to be explainable by design, and that requires treating transparency as an engineering requirement rather than a feature request.
Production-Ready Inference at Clinical Speed
Getting from a well-trained model to one that processes a full study in 41 milliseconds on standard GPU hardware requires optimisation work that most AI development stops short of. Mixed precision training, ensemble architecture, and hardware-specific tuning are the difference between a benchmark result and a system a radiologist can actually use in a shift.
End-to-End Delivery From Model to Clinical Interface
Akoode built the full Sahayak platform: deep learning models, training pipeline, Grad-CAM explainability layer, automated triage logic, and the dual-mode Streamlit clinical interface. One team, one brief, no integration gap between the AI and the tool the clinician opens.